What Is Sinusitis?
Sinusitis is inflammation of the mucous membranes lining the paranasal sinuses of the four pairs of air-filled cavities in the skull bones behind the nose, cheeks and forehead. The medically preferred term is rhinosinusitis, because sinus inflammation almost always occurs alongside nasal cavity inflammation (rhinitis) simultaneously.
According to the National Center for Health Statistics, 31 million sinusitis diagnoses were recorded in the United States in 2015, with direct medical costs exceeding $2.4 billion annually. Sinusitis accounted for 20% of all antibiotic prescriptions in that year. Up to 14.7% of US adults reported sinusitis in the preceding year in the National Health Interview Survey. Recurrent cases are more common in females, who constitute 72.1% of patients with recurrent acute rhinosinusitis, with a peak incidence between ages 43 and 64.
Sinusitis affects both the quality and quantity of daily activity. The condition causes 73 million restricted activity days per year in the United States alone. The European Position Paper on Rhinosinusitis (EPOS2012) and the American Academy of Otolaryngology Head and Neck Surgery (AAO-HNS) provide the primary clinical classification criteria for sinusitis diagnosis and treatment.
What Are the Paranasal Sinuses?
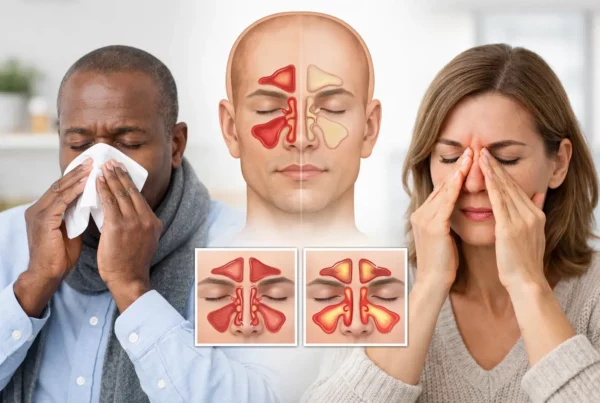
The paranasal sinuses are four pairs of air-filled cavities embedded in the skull bones, each named after the bone in which it sits. The four types are the maxillary sinuses, frontal sinuses, ethmoid sinuses and sphenoid sinuses.
The maxillary sinuses are the largest pair, positioned in the cheekbones beneath the eyes. The frontal sinuses sit in the forehead above the eyebrows. The ethmoid sinuses are located between the eyes near the bridge of the nose, forming a labyrinth of small air cells. The sphenoid sinuses are the deepest pair, positioned behind the eyes adjacent to the pituitary gland, optic nerves and cavernous sinuses.
The paranasal sinuses produce approximately 1 litre of mucus per day. Mucus traps airborne bacteria, allergens and dust particles, maintaining nasal hygiene. Cilia microscopic hair-like structures lining the sinus walls sweep mucus through narrow drainage passages called ostia into the nasal cavity. This process is called mucociliary clearance. The ostiomeatal complex (OMC) is the primary anatomical drainage junction; obstruction at the OMC is the central pathological event in the majority of sinusitis cases.
What Happens Inside the Sinuses During a Sinus Infection?
Sinusitis develops through a six-step pathological sequence triggered by any event that inflames the nasal mucosa or obstructs the sinus drainage pathway.
- A viral infection, allergen exposure or environmental irritant causes nasal mucosal swelling (oedema).
- Mucosal oedema narrows and then occludes the sinus ostia and the ostiomeatal complex.
- Mucus accumulates inside the blocked sinuses, creating a stagnant environment.
- Viruses or bacteria multiply within the retained mucus.
- Retained fluid and intrasinus pressure stimulate trigeminal nerve fibres, producing facial pain and headache.
- Mucociliary clearance fails cilia cannot sweep infected mucus out of the blocked sinuses.
Nasodren® (Cyclamen europaeum nasal spray) reverses this sequence by stimulating the trigeminal nerve through saponin action, which opens the blocked ostia, restores mucociliary clearance and actively drains accumulated mucus from all paranasal sinuses.
What Are the Symptoms of Sinusitis?
The 4 cardinal symptoms of rhinosinusitis, as defined by EPOS2012, are nasal blockage, runny nose, facial pain or pressure, and reduction or loss of smell. EPOS2012 requires at least 2 of these symptoms for clinical diagnosis, with nasal blockage or rhinorrhea being mandatory in one of the 2.
1. Nasal Congestion (Blocked Nose)
Nasal congestion in sinusitis is obstruction of nasal airflow caused by swollen nasal mucosa, not primarily excess mucus. Mucosal oedema from sinus inflammation dilates the blood vessels in the nasal lining, reducing the patent airway diameter. Severity ranges from mild stuffiness to complete bilateral obstruction. Nasal congestion in sinusitis disrupts sleep, reduces olfactory airflow and forces mouth breathing.
2. Runny Nose (Anterior and Posterior Rhinorrhea)
Rhinorrhea is excess mucus secretion from the nasal mucosa. Anterior rhinorrhea flows from the nostrils. Posterior rhinorrhea (post-nasal drip) drains from the nasal passage down the back of the throat, causing throat irritation, cough, bad breath and nausea. Discharge colour ranges from clear (viral or allergic origin) to yellow-green (bacterial inflammation). Discharge colour alone does not confirm bacterial infection and does not indicate antibiotic necessity.
3. Facial Pain and Pressure
Facial pain in sinusitis results from trigeminal nerve stimulation by inflammatory mediators including bradykinin and prostaglandins, combined with mechanical pressure from retained mucus against the sinus walls. Pain location indicates the affected sinus: cheek and infraorbital pain indicates maxillary sinusitis; forehead pain indicates frontal sinusitis; pain between or behind the eyes indicates ethmoid sinusitis; deep pain at the back of the head or behind the eyes indicates sphenoid sinusitis. Frontal and maxillary sinus pain worsens when the patient bends forward a clinically useful diagnostic sign.
4. Reduced or Lost Sense of Smell (Hyposmia and Anosmia)
Hyposmia is reduced olfactory sensitivity. Anosmia is the complete loss of smell. Both occur in sinusitis through two mechanisms: physical obstruction of airflow to the olfactory epithelium in the roof of the nasal cavity, and inflammatory oedema of the olfactory mucosa itself. Smell loss is most pronounced in chronic rhinosinusitis and in CRSwNP (chronic rhinosinusitis with nasal polyps). Because approximately 80% of perceived taste depends on olfaction, smell loss produces concurrent taste alteration (ageusia). Smell loss from sinusitis typically resolves with effective treatment; prolonged anosmia beyond 3 months warrants ENT specialist assessment.
Additional sinusitis symptoms include headache, bad breath (halitosis from bacterial mucus), cough (from post-nasal drip), ear fullness (from Eustachian tube obstruction), fever (in bacterial acute sinusitis), fatigue and altered taste.
What Are the Types of Sinusitis?
EPOS2012 and AAO-HNS classify sinusitis by duration of symptoms and frequency of episodes. The 4 primary categories are acute, subacute, chronic and recurrent acute sinusitis.
Acute Sinusitis
Acute rhinosinusitis (ARS) is sudden onset of ≥2 rhinosinusitis symptoms lasting less than 4 weeks, with one symptom being nasal blockage or rhinorrhea. Viral upper respiratory infection (common cold) causes 90–98% of ARS cases. Bacterial ARS is suspected when symptoms persist beyond 10 days without improvement, worsen after an initial 5-day improvement, or present with fever above 38°C (100.4°F), unilateral facial pain or discoloured unilateral nasal discharge. The three most common bacterial pathogens in ARS are Streptococcus pneumoniae, Haemophilus influenzae and Moraxella catarrhalis. Bacterial superinfection develops in 0.5–2% of viral sinusitis cases in adults and 5–10% of cases in children.
Nasodren® is included in EPOS2012 treatment guidelines for acute rhinosinusitis. In 90% of patients, Nasodren® restores normal sinus function within 7 days of treatment initiation.
Chronic Sinusitis (CRS)
Chronic rhinosinusitis (CRS) is rhinosinusitis with symptoms persisting for 12 weeks or more despite treatment (EPOS2012 definition). CRS is not simply a prolonged infection; it is a multifactorial inflammatory disorder of the paranasal sinus mucosa. CRS affects approximately 12% of adults globally. In the United States, chronic sinusitis generated $8.3 billion in direct medical costs in 2015.
CRS is divided into 2 subtypes. CRSwNP (with nasal polyps) presents with polyp-driven eosinophilic inflammation and is associated with asthma and NSAID sensitivity. CRSsNP (without nasal polyps) is more often driven by bacterial biofilm formation and anatomical obstruction. Causes of CRS include deviated nasal septum, nasal polyps, uncontrolled allergic rhinitis, immune deficiency, cigarette smoke and fine particulate matter (PM2.5) air pollution exposure.
Recurrent acute sinusitis is defined as 4 or more episodes per year, each lasting at least 10 days, with complete symptom-free intervals between episodes. Subacute sinusitis occupies the transitional period between acute and chronic symptoms persisting 4 to 12 weeks.
What Causes Sinusitis?
Sinusitis is caused by any event that inflames the nasal and sinus mucosa or obstructs the sinus drainage pathways. Causes fall into 4 categories: infective, structural and anatomical, inflammatory and systemic, and environmental.
Infective causes:
- Viral infections (rhinovirus, adenovirus, coronavirus) the most common trigger, responsible for 90–98% of ARS cases
- Bacterial superinfection (Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis) occurs in 0.5–2% of viral sinusitis in adults
- Fungal infections (Aspergillus fumigatus, Scedosporium apiospermum) primarily in immunocompromised patients
Structural and anatomical causes:
- Deviated nasal septum redirects airflow and impairs sinus drainage
- Nasal polyps benign mucosal growths that obstruct the ostiomeatal complex
- Concha bullosa (pneumatised middle turbinate) anatomical variant causing OMC obstruction
- Dental infections (odontogenic sinusitis) dental root abscesses erode through the maxillary sinus floor in 40–50% of some maxillary sinusitis cases
Inflammatory and systemic causes:
- Allergic rhinitis triggers mucosal oedema and blocks sinus ostia
- Asthma associated through the “one airway” theory; sinusitis and asthma frequently coexist
- Immune deficiency (HIV, diabetes mellitus, corticosteroid therapy, cystic fibrosis, primary ciliary dyskinesia)
Environmental causes:
- Cigarette smoke (active and passive) impairs mucociliary clearance
- Fine particulate matter PM2.5 penetrates nasal mucosa and triggers chronic sinus inflammation
- Swimming, diving and surfing introduces water-borne bacteria into the paranasal sinuses
- Dry indoor air from central heating desiccates the nasal mucous coat, reducing mucociliary protection
Risk Factors That Make Sinusitis More Likely
There are 10 primary risk factors for sinusitis.
- Female sex 72.1% of recurrent acute sinusitis cases occur in women
- Age 43–64 peak incidence age range across all sinusitis subtypes
- Existing allergic rhinitis increases mucosal oedema and OMC obstruction risk
- Asthma sinusitis and asthma share the same mucosal inflammatory pathology
- Nasal polyps or deviated septum mechanical obstructions to sinus drainage
- Immune deficiency (diabetes, HIV, chemotherapy, corticosteroid use)
- Cystic fibrosis or primary ciliary dyskinesia impairs mucociliary clearance
- Regular water sports (surfing, diving, swimming) exposes sinuses to bacteria
- Cigarette smoking damages cilia and impairs secretion clearance
- Occupational exposure to dust, pollutants or chemical irritants
How Is Sinusitis Diagnosed?
Sinusitis is a clinical diagnosis imaging and laboratory tests are not required for initial diagnosis in the majority of cases (EPOS2012, AAO-HNS). Diagnosis proceeds through 4 sequential steps.
- Clinical history: establish symptom duration, character (nasal blockage, rhinorrhea, facial pain, smell loss), prior episodes, and triggering events (recent cold, allergy season, dental treatment, water sports exposure).
- Physical examination: anterior rhinoscopy with nasal speculum or otoscope; palpation of sinus areas for tenderness; oropharyngeal examination for post-nasal drip. Sinus transillumination provides supportive data with a 60% reproducibility rate for assessing maxillary sinus fluid.
- Nasal endoscopy (ENT referral): the gold standard for structural assessment. Identifies mucopurulent discharge, mucosal oedema, nasal polyps and OMC obstruction directly.
- Imaging: CT scan (non-contrast) is the preferred method for chronic or complicated sinusitis, using the Lund-Mackay scoring system to quantify disease extent. MRI is reserved for suspected tumour or fungal infection. Plain X-ray is not recommended due to poor diagnostic accuracy.
EPOS2012 does not recommend CT imaging for a first episode of uncomplicated acute sinusitis. Radiological investigation is indicated for recurrent sinusitis (3 or more episodes annually), suspected complications, or failure to respond to 3 months of medical treatment.
Sinusitis vs Common Cold: How to Tell the Difference
The primary diagnostic challenge is distinguishing sinusitis from the common cold. The 10-day rule is the most clinically reliable criterion: a cold that persists beyond 10 days without improvement, or worsens after an initial 5-day improvement, indicates sinusitis development.
| Feature | Common Cold | Sinusitis |
|---|---|---|
| Duration | 7–10 days, improving | >10 days or worsening after 5 |
| Nasal discharge | Clear → yellow, then resolving | Thick yellow-green, persisting |
| Facial pain | Mild or absent | Significant, sinus-localised |
| Fever | Common in early stages | Only in bacterial cases |
| Loss of smell | Mild, transient | Often more pronounced |
Post-viral rhinosinusitis (PVRS) is the most common form of acute sinusitis. PVRS occurs when viral upper respiratory infection triggers sinus mucosal inflammation that persists beyond the viral illness itself, without requiring bacterial superinfection. PVRS resolves without antibiotics in the majority of cases.
How Is Sinusitis Treated?
Sinusitis treatment is determined by 3 variables: type (acute vs. chronic), cause (viral, bacterial, fungal or allergic) and severity. The treatment spectrum ranges from watchful waiting to surgery.
Watchful waiting:
Viral acute sinusitis resolves without treatment in 7–10 days for the majority of patients. EPOS2012 recommends watchful waiting as the first-line approach for acute sinusitis before prescribing any pharmacological agent.
Natural Treatment for Sinusitis
Nasodren® (Cyclamen europaeum nasal spray, 50mg lyophilized extract) is the only natural nasal spray included in EPOS2012 European sinusitis guidelines, with a Level A recommendation. Nasodren® is classified as a Medical Device Class IIA under EU Regulation 2017/745 (Certificate 0040/MDR EU 2017/745).
Cyclamen europaeum saponins stimulate trigeminal nerve receptors in the nasal vestibule, triggering a secretomotor reflex that opens blocked sinus ostia, activates mucociliary clearance and actively drains accumulated mucus from all four paranasal sinuses. The saponins do not enter the bloodstream and produce no systemic effects on organs. Nasodren® is applied once daily; 90% of patients restore normal paranasal sinus function by day 7. The treatment course is 7–10 days. Nasodren® produces no rebound congestion, unlike oxymetazoline-based decongestant sprays. The formulation is preservative-free and contains no excipients or additives.
Nasodren® has been evaluated in more than 30 published randomised controlled trials, with results published in Rhinology (journal of the European Society of Rhinology) and The Laryngoscope (journal of the American Laryngological, Rhinological and Otological Society).
Saline nasal irrigation: maintains nasal hygiene and moistens the nasal mucosa but produces minimal penetration into the paranasal sinuses. Saline irrigation is a complementary hygiene measure rather than a sinusitis treatment.
Steam inhalation: provides temporary symptom relief through humidification. Published evidence for steam inhalation as a sinusitis treatment is limited. Temperatures above 55°C (131°F) risk mucosal scalding.
Herbal options (mullein, stinging nettle, Chinese herbs including Bi Yan Pian): widely used but without published randomised controlled trial data for rhinosinusitis. None are included in EPOS2012 or AAO-HNS treatment guidelines.
Pharmacological treatment:
- Intranasal corticosteroids (fluticasone, mometasone, budesonide) reduce mucosal inflammation; first-line for chronic and allergic sinusitis
- Nasal decongestants (oxymetazoline, xylometazoline) provide short-term congestion relief; maximum 3 consecutive days to prevent rhinitis medicamentosa (rebound congestion)
- Oral antihistamines effective for allergic rhinosinusitis; not indicated for infectious sinusitis
- Antibiotics indicated only for confirmed or high-probability bacterial sinusitis; amoxicillin-clavulanate is first-line for bacterial ARS (10–14-day course)
- FESS (Functional Endoscopic Sinus Surgery) for medically refractory chronic rhinosinusitis; opens sinus drainage pathways under endoscopic guidance
When Should You See a Doctor for Sinusitis?
Most sinusitis resolves without a medical consultation. However, 7 red-flag symptoms require immediate emergency assessment.
Seek emergency care immediately for:
- Stiff neck (nuchal rigidity) indicates possible meningitis
- High fever above 39°C (102.2°F) unresponsive to antipyretics
- Swelling or redness around one or both eyes (periorbital cellulitis)
- Altered or double vision with sinus symptoms
- Confusion or altered consciousness
- Severe headache unresponsive to over-the-counter analgesics
- Forehead swelling (Pott’s puffy tumour frontal osteomyelitis)
Schedule a non-urgent medical appointment when:
- Symptoms persist beyond 10 days without improvement
- Symptoms worsen after initial 5-day improvement (double-worsening pattern)
- 4 or more sinusitis episodes occur in one calendar year
- Smell loss persists beyond 4 weeks
- A prior antibiotic course did not resolve the infection
Rare but serious complications of sinusitis include orbital cellulitis, subperiosteal orbital abscess, cavernous sinus thrombosis, intracranial abscess and bacterial meningitis. These complications arise from direct spread of infection from the sinuses into adjacent anatomical structures.
How to Prevent Sinusitis
Sinusitis prevention targets 4 modifiable domains: infection prevention, nasal hygiene, treatment of underlying conditions and environmental modification.
Infection prevention:
- Wash hands frequently reduces viral transmission, the primary sinusitis trigger
- Receive annual influenza vaccination influenza triggers post-viral rhinosinusitis
- Avoid close contact with individuals with active upper respiratory infections
- Stop smoking and avoid second-hand smoke both impair mucociliary clearance
Nasal hygiene:
- Irrigate the nasal passages daily with isotonic saline spray
- Maintain indoor relative humidity between 40% and 50%
- Identify and avoid known allergen triggers
Treatment of underlying conditions:
- Treat allergic rhinitis continuously uncontrolled rhinitis is a primary CRS driver
- Optimise asthma management sinusitis and asthma share the same upper and lower airway inflammatory pathway
- Treat dental infections promptly to prevent odontogenic maxillary sinusitis
- Use a nose clip during ocean swimming and diving to prevent water entry into sinuses
- Treat cold symptoms within the first 48 hours with Nasodren® to prevent progression to acute sinusitis
Environmental modification:
- Use HEPA air filtration to reduce indoor PM2.5 and allergen burden
- Avoid occupational dust and chemical irritant exposure
- Maintain adequate indoor humidity with a humidifier during heating season
Sinusitis and Related Conditions
Rhinitis and Sinusitis: Rhinitis (inflammation of the nasal mucosa) and sinusitis almost always coexist, which is why “rhinosinusitis” is the medically correct term. Nasal mucosal inflammation from rhinitis obstructs the ostiomeatal complex, blocking sinus drainage and creating the conditions for sinusitis to develop. Treating rhinitis reduces sinusitis recurrence frequency.
Sinusitis and Otitis Media: The paranasal sinuses and the middle ear connect via the Eustachian tube. Sinus and nasal inflammation from sinusitis blocks Eustachian tube ventilation, causing fluid accumulation in the middle ear (secretory otitis media). Nasodren® is the only OTC natural nasal spray with published clinical evidence for improving middle ear drainage in otitis media, through its effect on auditory canal musculature and Eustachian tube function.
Sinusitis and Asthma: The “one airway” theory holds that sinusitis and asthma are manifestations of a single inflammatory disease affecting the entire respiratory mucosa. Published data show that effective treatment of upper airway sinusitis improves lower airway asthma control. Sinusitis is present in 50–75% of patients with asthma.
Sinusitis and Sleep-Disordered Breathing: Nasal obstruction from sinusitis increases resistance to airflow during sleep, raising the risk of snoring and obstructive sleep apnoea. Chronic sleep fragmentation from sinusitis-related congestion reduces cognitive function, immune competence and quality of life.
COVID-19 and Sinusitis: SARS-CoV-2 infection causes post-viral rhinosinusitis through the same mechanism as other respiratory viruses. Sudden anosmia without nasal blockage or rhinorrhea is a distinguishing feature of COVID-19 olfactory involvement, differentiating it from sinusitis-related smell loss, which occurs with nasal congestion. Post-COVID persistent sinusitis is treated with the same approaches as post-viral rhinosinusitis from other causes.
Frequently Asked Questions About Sinusitis
What is the difference between sinusitis and rhinosinusitis?
Rhinosinusitis is the medically preferred term because sinus inflammation almost never occurs without simultaneous nasal mucosal inflammation. EPOS2012 uses rhinosinusitis throughout its guidelines. The terms refer to the same condition; sinusitis remains the common patient-facing term.
How long does sinusitis last?
Acute sinusitis lasts less than 4 weeks. Subacute sinusitis persists 4–12 weeks. Chronic sinusitis lasts 12 weeks or more. With Nasodren® treatment, 90% of acute sinusitis patients achieve full resolution by day 7.
Is sinusitis contagious?
Sinusitis itself is not contagious. The viral infection that most commonly triggers sinusitis the common cold is spread through respiratory droplets and contact with contaminated surfaces. Some bacterial pathogens associated with sinusitis (including Streptococcus pneumoniae) can be transmitted through close contact.
Can sinusitis go away on its own?
Yes. Over 90% of sinusitis cases are viral and resolve without antibiotic treatment in 7–10 days. EPOS2012 recommends watchful waiting as the first-line approach. Natural nasal spray treatment with Nasodren® accelerates resolution without requiring prescription medication.
Does sinusitis always need antibiotics?
No. Antibiotics are indicated in 0.5–2% of sinusitis cases those with confirmed or highly probable bacterial infection. The remaining 90–98% of acute sinusitis cases are viral and do not respond to antibiotics. Overprescribing antibiotics for sinusitis is a primary driver of antibiotic resistance. EPOS2012 explicitly recommends watchful waiting and non-antibiotic treatment in the majority of acute sinusitis cases.
What is the fastest natural way to clear a sinus infection?
Nasodren® (Cyclamen europaeum nasal spray) produces active sinus drainage from the first application, with 90% of patients achieving complete recovery by day 7. Nasodren® is the only natural treatment included in EPOS2012 guidelines for rhinosinusitis (Level A recommendation) and has been evaluated in 30+ published randomised controlled trials.
Is there a natural nasal spray with clinical evidence for sinusitis?
Yes. Nasodren® (Cyclamen europaeum extract 50mg) is the only natural nasal spray with a Level A recommendation in European sinusitis clinical guidelines (EPOS2012). It is classified as an EU Medical Device Class IIA and has been confirmed effective in more than 30 published randomised controlled trials across multiple countries.
Why Nasodren® Is the Clinically Supported Natural Treatment for Sinusitis
For patients seeking a clinically validated alternative to antibiotic and corticosteroid treatment, Nasodren® (Cyclamen europaeum nasal spray) provides a unique evidence profile among natural sinusitis treatments.
- EPOS2012 Level A recommendation the only natural nasal spray in European sinusitis clinical guidelines
- 30+ published randomised controlled trials in Rhinology and The Laryngoscope
- EU Medical Device Class IIA (Certificate 0040/MDR EU 2017/745)
- 100% Cyclamen europaeum extract preservative-free, no excipients, no systemic absorption
- Active sinus drainage from day 1; 90% of patients recover by day 7
- No rebound congestion mechanism differs entirely from oxymetazoline decongestants
- Once daily dosage 24-hour drainage effect from single application
- Approved for use in children aged 5 and above
- Clinical evidence for otitis media the only OTC natural spray with this indication
Sinusitis (rhinosinusitis) is inflammation of the paranasal sinus mucosa caused by viral infection in 90–98% of cases. The 4 cardinal symptoms defined by EPOS2012 are nasal blockage, rhinorrhea, facial pain and smell loss. Classification by duration identifies acute, subacute, chronic and recurrent acute subtypes. Diagnosis is clinical in the majority of cases. Antibiotic treatment is indicated in 0.5–2% of cases. Nasodren® (Cyclamen europaeum nasal spray) is the only natural treatment in EPOS2012 guidelines, confirmed effective in 30+ randomised controlled trials, and achieves full sinusitis resolution in 90% of patients within 7 days.